



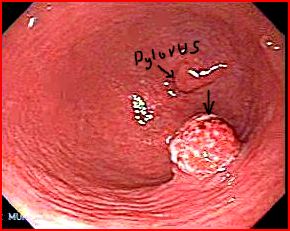
Mr Barrett, a 50 year old HGV driver had an endoscopy performed for symptoms of dyspepsia. The endoscopy showed:

What is the diagnosis?
Gastric polyp in the antrum
This is an incidental finding
What are the types of gastric polyps?
- Hyperplastic (3/4 of all polyps)
- Adenomatous
- Inflammatory
What are the clinical features of gastric polyps?
Gastric polyps are mostly asymptomatic and are typically found incidentally at OGD. GI bleed (usually occult) can happen rarely.
Discuss hyperplastic polyps?
Hyperplastic polyps are caused by an inflamed and often atrophic gastric mucosa. These polyps typically occur in the antrum and often in presentations of multiple lesions. In larger hyperplastic polyps, the surface epithelium is often eroded. This erosion may result in chronic blood loss and iron deficiency anaemia. It occurs due to a hyper proliferative response to tissue injury (erosions or ulcers), caused by NSAIDS, H. Pylori etc.
Discuss the management of hyperplastic polyps?
Removal of underlying injury (i.e. eradication of H. Pylori infection) results in regression of up to 70% of hyperplastic polyps. A repeat OGD should be done a few months after eradication to monitor not only cure of the infection, but also recurrence or regression of remaining polyps.
Hyperplastic polyps have a low but definite potential for development of malignancy. The overall prevalence of dysplasia is estimated at less than 2%; however, the risk is higher if polyps exceed 2 cm in size. For this reason, large polyps must be completely excised for thorough histological evaluation.
Discuss adenomatous polyps?
Adenomatous polyps are usually solitary polyps (sessile or pedunculated) located in the antrum. These polyps are most often associated with chronic atrophic gastric metaplasia, and they have a defined cancer risk. The larger the polyp, the greater the risk that the polyp contains cancer. In polyps larger than 2 cm, the risk for cancer is as high as 50%. Endoscopic resection is appropriate. The guidelines of the American Society of Gastrointestinal Endoscopy (ASGE) recommend surveillance endoscopy one year after removing adenomatous gastric polyps to assess recurrence at the prior excision site.
Discuss inflammatory polyps?
Inflammatory polyps are rare, representing less than 1% of all gastric polyps. These polyps are rarely symptomatic but can be associated with bleeding. Most inflammatory fibroid polyps are found incidentally. The aetiology of inflammatory fibroid polyps is unknown. As inflammatory fibroid polyps do not recur after excision, neither further treatment beyond local excision nor surveillance is recommended.
Discuss the management of the polyp in the current case?
The polyp was removed endoscopically. The histology showed hyperplastic polyp.
Remember: Polyps may be difficult to retrieve in stomach as it can drop through the pylorus and be eliminated by rapid passage through the small intestine. Thus, an adequate biopsy sample should be obtained prior to polypectomy.
Ref:
Image courtesy of www.gastrointestinalatlas.com

