



Anti reflux surgery
What are the indications for antireflux surgery?
- Regurgitation-dominant or volume related reflux symptoms (although there is no proven superiority for surgery for this indication)
- Persistent or recurrent symptoms despite PPI therapy
- Dissatisfaction at continuing long term PPI
- Poor compliance (for example due to costs of PPI)
- Presence of large hiatus hernia
Discuss the principles of anti reflux surgery?
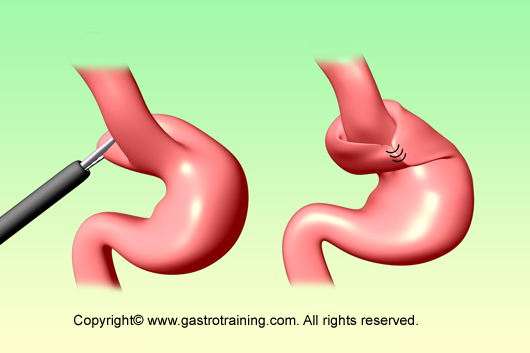
Anti reflux surgery focuses on restoring a physiologic equivalent to the normal lower oesophageal sphincter. Nissen fundoplication is the most common anti reflux surgery performed. Here, fundus of the stomach is passed around the lower part of the oesophagus and is sutured onto itself to form a 360 degree wrap of stomach around the lower oesophagus
The Nissen fundoplication is total (360 degree), but partial fundoplications known as Belsey fundoplication (270 degree), Dor fundoplication (anterior 180 degree) or Toupet fundoplication (posterior 180 degree) are other alternative procedures.
Discuss the pros and cons of anti reflux surgery?
- Most antireflux surgery is now performed laparoscopically with short duration of hospital stay (1-2 nights) and faster recovery (resume work in 1-2 weeks).
- 85-90% success rates in relieving symptoms and healing oesophagitis.
- 10 to 65 percent of patients still required some form of antisecretory medications after surgery
- Surgery is not superior to medical therapy in preventing complications of GORD such as stricture formation, development or progression of Barrett’s oesophagus, or development of adenocarcinoma.
Discuss complications of anti reflux surgery?
Major complications are uncommon. Complications are:
- Dysphagia: postoperative dysphagia is not uncommon, but eases off within a few weeks. Dysphagia that persists requires further evaluation. Some may need dilatation; however patients with Nissen fundoplication may need revision to a partial fundoplication if dysphagia persists.
- Gas bloat syndrome (bloating with inability to belch) – symptoms gradually improve. Prokinetic agents may help
- Rectal flatulence
- Other complications- fundal wrap can become undone leading to recurrence of symptoms, wrap can slip into the chest (causing dysphagia and vomiting) – diagnosis is made by barium swallow and CXR shows a gastric bubble above the diaphragm.
- Complications during surgery- gastric or oesophageal injury, splenic injury, pneumothorax etc
http://www.youtube.com/watch?v=Bi5C7-OdYAs&feature=fvw (schematic diagram)

