



Mr Nixon, a 45 year old company executive presents with progressive dysphagia to solids and liquids for 3 months. He suffers from GORD and has been using PPI intermittently. His endoscopy showed:
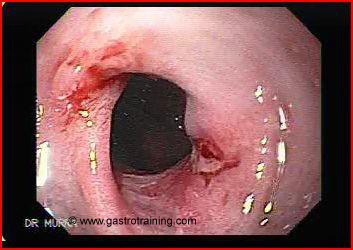
What is the diagnosis?
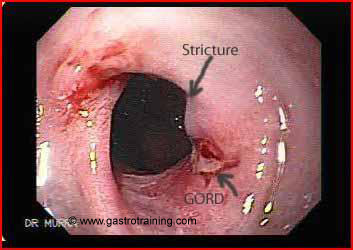
Benign oesophageal stricture secondary to GORD. It did not allow the scope to pass through
Discuss the next steps?
The stricture should be biopsied to exclude malignancy
Long term PPI
Repeat endoscopy after 6-8 weeks. PPI therapy often heals the inflammation and the stricture improves. If the stricture persists at repeat endoscopy- dilatation will be needed.
What are the causes of oesophageal stricture?
The majority of oesophageal strictures are reflux related. Other causes are malignancy, anastomotic, sclerotherapy, radiation, medication, and corrosive induced strictures, and rings and webs.
Eosinophilic oesophagitis is a recently described emerging cause of oesophageal stricture.
What is the diameter to which the obstruction should be dilated?
Dysphagia occurs when the oesophageal diameter is less than 13 mm. Thus a diameter of 13-15mm is generally accepted as the end point of dilatation. A few patients will require greater diameters for symptom relief.
Further reading
Link to Benign oesophageal stricture
Link to Benign oesophageal dilatation
Image courtesy of www.gastrointestinalatlas.com

