
Device assisted enteroscopy
Small bowel is 17feet (5-6Metres) long and large bowel is 5feet (1.5Metre) long
Double balloon enteroscopy (DBE) is a new diagnostic and therapeutic modality originally described by Yamamoto et al in 2001 that allows high resolution visualisation, diagnostic and therapeutic interventions in all segments of the small intestine. It came almost the same time as Video capsule endoscopy and at one point was thought to be each other competitors. However with more widespread use of VCE it is expected that roughly 10% of those patients will need enteroscopy for further evaluation or imparting therapy.
The double balloon enteroscope comprises a 145 cm overtube back loaded on a 200 cm enteroscope and a latex balloon attached to each end.
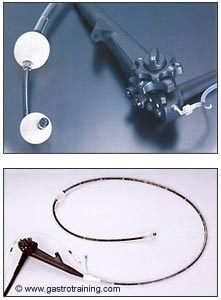
(courtesy-http://www.fujinonendoscopy.com)
Technical details
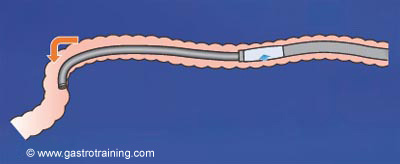
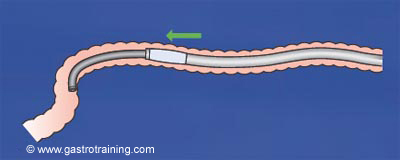
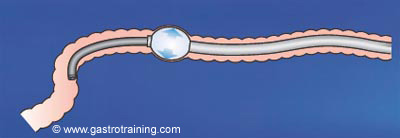
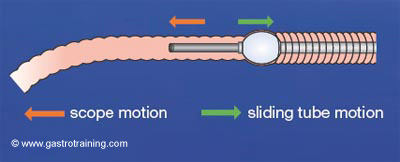
- Once the system is passed into the proximal small bowel, the balloon of the overtube is inflated to anchor the position, so that the endoscope can be advanced. When the endoscope is advanced to its most distal point, the endoscope balloon is inflated to hold the insertion point. The overtube can be advanced after deflating the overtube balloon. This serial inflation and deflation of balloons allow pleating of bowel on the back of the overtube and forward advancement of the enteroscope into a new segment of bowel. This process is repeated until advancing the endoscope any further becomes difficult.
- DBE can be used both from the mouth (anterograde approach) and anus (retrograde approach). The insertion route can be chosen according to the estimated location of the suspected lesions. Stable advancement of the enteroscope into the ileum from the anal approach is particularly challenging and failures occur in about 20% of patients
- The procedure can generally be performed under conscious sedation ( with midazolam/fentanyl) but general anaesthesia is preferrable.The entire small bowel can be visualized in 80 to 90 percent of cases (but requires significant experience of over 150 cases), with lesser degrees of visualization in patients who are obese and in operators with less experience with DBE (1).
- Screening is helpful in initial stages of learning and nice concentric circle with three turns normally ensures the tip is in sight of the target.
- Panenteroscopy is generally achieved by a combination of both the antegrade (oral) and retrograde (rectal) approach. In rare situations, panenteroscopy can be achieved via a single (oral or rectal) approach. Panenteroscopy is demonstrated by India ink injection at the most distal site during antegrade (or retrograde) DBE and by successful advancement of the enteroscope to the tattooed area during the opposite approach.
- The mean duration of the procedure varies from 90-120 minutes depending on the operator experience.
Indications
The main indications are
- Investigation of gastrointestinal bleeding and inflammatory bowel disease.
- Evaluation of abnormal capsule endoscopy or abnormal radiographic studies
Other indications for DBE include an evaluation of suspected small-bowel diarrhoea, abdominal pain, the removal of small-bowel polyps, treatment for angiodysplasias (APC) or small intestinal bleeding ( Endoclip) ,the retrieval of tissue samples/ stuck capsule and accessing ampulla for ERCP in Roux-en-Y anastomoses, post bariatric surgery, small intestinal stricture dilatation/ stenting, tattooing to assist laparoscopic small bowel resection. Difficult colonoscopy is another indication when rectal approach is used.
One important point is if APC is used to treat any telangiectasia in small bowel – Argon flow is to be reduced to 1.5 litres/minute (normally 2 litres/minute) and energy reduced to A30 (normally A65 for Stomach/duodenum). Also avoid physical contact of the small bowel wall with the tip of APC catheter as suddenly the wall can be blown up with the gas. Also to inflate CO2 should be preferentially used.
Limitations
The limitations of DBE include the long procedural time and the patient discomfort and increased need for sedation.
Complications
Diagnostic DBE has an overall complication rate of 1.7% (perforation 0.3%, bleeding 0.8%, pancreatitis 0.3%). The cause of pancreatitis is uncertain. Therapeutic DBE has a relatively high complication rate of 4.3% (polypectomy bleeding 3.3%, argon plasma coagulation perforation 1.2%, dilation perforation 2.9%) (2).
Single balloon enteroscopy
Single balloon enteroscopy (SBE) is similar to DBE except that SBE utilizes a single balloon on the overtube and a hyper flexible endoscope tip. Rather than the balloon at the tip of the endoscope fixing the endoscope when overtube is advanced- the intestine is fixed by hooking the flexible distal tip (J manoeuvre).
- Insert the scope as deep as possible into the small bowel and fix the angulation of the scope.
- Advance the overtube.
- Inflate the balloon.
- Withdraw the overtube and if possible, try to push the endoscope simultaneously.

(courtesy-http://www.olympus.com)
This decreases set-up time and also no assistant is needed. The single balloon enteroscope is also stiffer that may facilitate one-to-one advancement in the small bowel and improve success rates for ileal intubation from the anal approach. In the initial clinical experience using SBE, average depth of insertion (270 cm) and diagnostic yield (54%) were similar to those with DBE (3).Procedure time was somewhat shorter. There are no comparison studies between DBE and SBE with regard to complete enteroscopy rates.
Previously Enteroscopy was done either by Push Enteroscopy or Sonde enteroscopy
Push Enteroscopy
Push enteroscopy is an endoscopic procedure whereby a longer endoscope is inserted into the jejunum through the mouth to evaluate a larger segment of the small bowel. The diagnostic yield of push enteroscopy is approximately 40% to 65%.
Push enteroscopy is normally done with a paediatric colonoscope +/- overtube. The main disadvantage is the fact that small bowel is too long and being supported on a mobile mesentery, the endoscope tends to accentuate the natural curvature and makes complete examination almost impossible.
Sonde enteroscopy
Sonde enteroscopy involves the use of a long, flexible, fiberoptic instrument propelled through the small bowel by peristalsis; this procedure may allow for viewing the remainder of the small bowel. Sonde instruments rely on a balloon placed at the instrument’s tip. Peristalsis then advances the long flexible endoscope to the distal small bowel, and the endoscopic examination is performed during withdrawal. In contrast to push enteroscopy, this instrument has no biopsy or therapeutic capability.
References
- Gross SA, Stark ME. Initial experience with double-balloon enteroscopy at a U.S. center. Gastrointest Endosc 2008; 67:890-897.
- Mensink PB, Haringsma J, Kucharzik T, et al. Complications of double balloon enteroscopy: a multicenter survey. Endoscopy 2007; 39:613-615.
- Tsujikawa T, Saitoh Y, Andoh A, et al. Novel single-balloon enteroscopy for diagnosis and treatment of the small intestine: preliminary experiences. Endoscopy 2008; 40:11-15.
Article printed from Gastroenterology Education and CPD for trainees and specialists: https://www.gastrotraining.com